Four proposed Categories of Möbius Syndrome
1. Group I: Characterized by small or absent brain stem nuclei that control the cranial nerves
2. Group II: Characterized by loss and degeneration of neurons in the facial peripheral nerve
3. Group III: Characterized by loss and degeneration of neurons and other brain cells; microscopic areas of damage, and hardened tissue in the brainstem nuceli
4. Group IV: Characterized by muscular symptoms in spite of lack of lesions in the cranial nerve.
2. Group II: Characterized by loss and degeneration of neurons in the facial peripheral nerve
3. Group III: Characterized by loss and degeneration of neurons and other brain cells; microscopic areas of damage, and hardened tissue in the brainstem nuceli
4. Group IV: Characterized by muscular symptoms in spite of lack of lesions in the cranial nerve.
Diagnosis
Kumar, 1990
The first sign of Möbius syndrome in newborns is an inability to suck, sometimes with excessive drooling and strabismus (crossed eyes). In some patients, at birth we see abnormalities of the limbs, tongue, and jaw. Children can also have decreased muscle tone in the upper limbs as well as a lack of facial expression. (Pollin, 2010). Later it is seen that children with Möbius syndrome do not smile or move their facial muscles when crying (Kumar, 1990).
CRITERIA FOR DIAGNOSIS
1. Complete or partial facial nerve paralysis
2. Limb Malformations often are present
3. Additional clinical features in association with complete or partial facial nerve (VII) paralysis may be present:
CRITERIA FOR DIAGNOSIS
1. Complete or partial facial nerve paralysis
2. Limb Malformations often are present
3. Additional clinical features in association with complete or partial facial nerve (VII) paralysis may be present:
- Bilateral or unilateral ocular nerve palsies (of abducens (VI)) and less commonly of the oculomotor (III) and trochlear (IV) nerves
- Hypoplasia of the tongue due to the hypoglossal (XII) nerve paralysis
- Swallowing and speech difficulties due to tirgeminal (V), glosspharyngeal (IX), and vagus (X) nerve palsies
- Malformations of the orofacial structures
- Other anomalies of the musculoskeletal system
Other Names for Möbius Syndrome
Möbius syndrome is also known as:
- Congenital facial diplegia
- Congenital opthalmoplegia and facial paresis
- Möbius sequence
- Möbius congenital oculofacial paralysis
- Möbius spectrum
Symptomology
Symptoms may include:
- Lack of facial expression; inability to smile
- Feeding, swallowing and choking problems
- Keeping head back to swallow
- Eye sensitivity due to inability to squint
- Motor delays due to upper body weakness
- Absence of lateral eye movement
- Absence of blinking
- Strabismus (crossed eyes)
- Drooling
- High palate
- Short or deformed tongue
- Submucous cleft palate
- Dental problems
- Hearing impairment
- Articulation/speech disorders
- Minor mid-line anomalies
- Club feet
- Hand/feet deformaties
Differential Diagnosis

The distribution of the facial weakness and lack of other associated palsies usually causes differentiated diagnosis. The craniofacial syndrome with assymmetric crying facies, congenital heart defects, and other factors may be confused with Möbius syndrome. In addition, other neuromuscular disorders such as infantile spinal muscular atrophy, congenital forms of Myasthenia Gravis, myotonic dystrophy, faciocapulohumoral dystrophy, and other myopathies may show initially during infancy (medlink). Additionally, the oromandibular-limb hypogenesis disorders overlap with Möbius syndrome due to the fact that disorders under that category are associated with limb and craniofacial abnormalities. A lot of the time children with Möbius can be mistaken for being mentally retarded, unfriendly, or rude. A full list of differential diagnoses are listed below:
There can be some difficulty in misdiagnosing children with Möbius at birth. Some cases that seem like Möbius may progress to a typical facio/scapulo/humoral muscular dystrophy and sometimes infantile myotonic dystrophy can resemble Möbius syndrome. However, bilateral abducens paralysis is not a feature of infantile myotonic dystrophy but it is a feature of Möbius syndrome. In addition, the infant's mothers are generally affected with myotonic dystrophy as well (Baraitser, 1977).
- Acquired facial palsy from delivery
- Cardiofacial syndrome with asymmetric crying facies
- Infantile spinal muscular atrophy
- Myasthenia gravis, congenital forms
- Myotonic dystrophy
- Metabolic neuropathy
- Facioscapulohumeral dystrophy
- Other myopathies
- Duane syndrome
- Oromandibular-limb hypogenesis disorders
- Hypoglossia-hypodactylia
- Hanhart syndrome
- Glossopalatine ankylosis
- Charlie M syndrome
- Athabascan brainstem dysgenesis syndrome
- Poland anomaly (absence of pectoralis major muscles)
- Klippel-Feil anomaly
There can be some difficulty in misdiagnosing children with Möbius at birth. Some cases that seem like Möbius may progress to a typical facio/scapulo/humoral muscular dystrophy and sometimes infantile myotonic dystrophy can resemble Möbius syndrome. However, bilateral abducens paralysis is not a feature of infantile myotonic dystrophy but it is a feature of Möbius syndrome. In addition, the infant's mothers are generally affected with myotonic dystrophy as well (Baraitser, 1977).
CLUFT Grading System
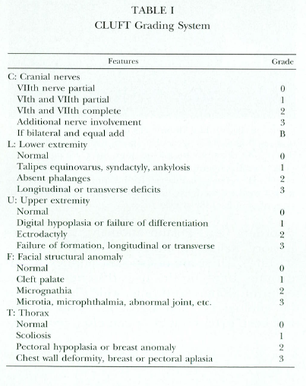
Abramson et. al, 1998
The table to the right is a stardard classification and grading system for diagnosing Möbius syndrome. This classification system was composed by a study with 27 patients from 1980-1994. Abramson and colleagues categorized and graded the cranial nerve deficits and diverse musculoskeletal abnormalities of the face, upper and lower limbs, and trunk. CLUFT stands for Cranial nerve, Lower limb, Upper limb, Face, and Thorax. These are each graded on a scale of 0 to 3 with 3 being the most severe. This grading system allows for a range of symptoms to be categorized by location and severity (Abramson et al, 1998).
References
- Abramson, D. L., M.D., Cohen, M. M., D.M.D., & Mulliken, J. B., M.D. (1997). Mobius Syndrome: Classification and Grading System. Division of Plastic Surgery and Craniofacial Centre at Childrens Hospital, Harvard Medical School, 102(4), 961-967.
- Banerjee, P. (2012). Moebius Syndrome. Retrieved April 22, 2013, from Hx Benefit Health Information website: http://www.hxbenefit.com/moebius-syndrome.html#moebius-syndrome-treatment
- Baraitser, M. (1977). Genetics of Mobius Syndrome. Journal of Medical Genetics, 14, 415-417.
- Holve S, Friedman B, Hoyme HE, et al. Athabascan brainstem dysgenesis syndrome. Am J Med Genet 2003;120A:169-73.
- Kumar, D. (1990). Moebius syndrome. Journal of Medical Genetics, 27, 122-126.
- Maccagno, A. (2013, March 16). Mobius Syndrome. Retrieved April 22, 2013, from Mobius Syndrome website: http://flipper.diff.org/app/items/info/5489
- Moebius Syndrome. (2013, April 16). Retrieved April 22, 2013, from Genetics Home Reference website: http://ghr.nlm.nih.gov/condition/moebius-syndrome#diagnosis
- Moebius Syndrome. (2010). Retrieved April 22, 2013, from Moebius Syndrome Global Information Site: http://www.moebiussyndrome.info/research/18-articles/13-mobius-syndrome
- Pollin, T. I. (2010). Moebius Syndrome. In L. J. Fundukian (Ed.), The Gale Encyclopedia of Genetic Disorders (3rd ed., Vol. 2, pp. 88-990). Detroit, MI: Gale Cengage Learning.
- What is Moebius Syndrome? (2007). Retrieved April 21, 2013, from Moebius Syndrome Foundation website http://www.moebiussyndrome.com/index.cfm?objectid=48F93851-BEFB-4468-999417A599ABAB5D
